|
|
Atypical Melanocytic proliferation, Not falling into a specific diagnostic category What does this mean? Dermatopathologists and diagnostic surgical pathologists would like their diagnostic world to fit into neatly defined categories but alas, we spend the majority of our time struggling with the diseases that do not fit. One category is the atypical melanocytic proliferation. These problematic cases sometimes become new diagnostic categories. Well known examples of this include animal type melanomas or the deep penetrating nevus. However, as we await other experts to proclaim a "new diagnostic entity", most of us still struggle with these as yet undefined entities. Sometimes the problem stems from cytological changes that are atypical, out of proportion to the lesion's usual morphology. One example could be a conventional melanocytic nevus that contains rare pleomorphic cells. Is this lesion a nevoid melanoma? Is the lesion not completely sampled? Is this a melanoma arising in association with a benign melanocytic nevus? What about an atypical dermal based melanocytic proliferation? Sometimes these lesions arise in the setting of a congenital nevus. Is this lesion a proliferative nodule or is this a melanoma in vertical invasive growth phase? (See figures 1-3 to the left). Although there are established histopathologic criteria to make the distinction, there are inevitably transitional forms that are vexing for any dermatopathologist. As with any diagnosis, the pathologist must clearly communicate the diagnostic concerns to the physician treating the patient. If the pathologist does not know how the lesion will behave, it must be clearly stated in the report. In most cases, a complete excision is usually recommended. Most of these diagnoses will be given with the following terminologies: Severely atypical melanocytic proliferation with features suspicious for evolving melanoma Clearly these are not definitive diagnoses but rather descriptors of the lesion, phrased to express the diagnostic concern over the cytology, architecture, or both. Although unsatisfying for both the treating physician and pathologist, the most important lesson is all parties understand this is a lesion with a guarded and uncertain prognosis, requiring complete removal and careful clinical follow-up. Submitted by Paul K. Shitabata, M.D. |
Last Updated
March 6, 2006
Send Emails to
Webmaster at DermpathMD
Read the Medical Disclaimer
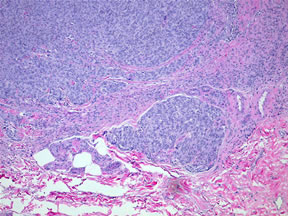
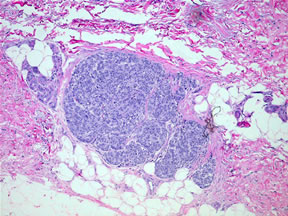
 Figure 3-Highest magnification showing moderate nuclear variabilty. A rare mitotic figure is identified. Is this a cellular proliferative nodule or invasive vertical growth phase melanoma?
Figure 3-Highest magnification showing moderate nuclear variabilty. A rare mitotic figure is identified. Is this a cellular proliferative nodule or invasive vertical growth phase melanoma?