Figure 1-Persistent plaque and patches on buttocks. Score 1 point for basic criteria and 1 for additional criteria of non-sun exposed location and variability in size and shape. Total 2 points.
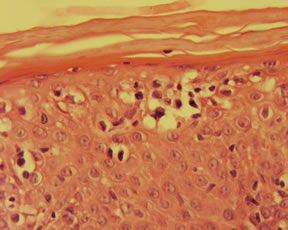
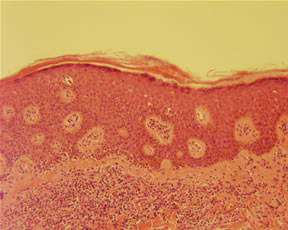
Total 2 points. Total summing the clinical and histopathological criteria: 4 points
|
The histopathologic diagnosis of mycosis fungoides is one of the most challenging areas in dermatopathology. The arrival of immunohistochemical stains and molecular gene rearrangment studies have aided in the diagnosis but ultimately it is a clinical-pathologic correlation, relying heavily upon conventional histomorphologic parameters. Recently, there have been concerted attempts to agree upon the histopathologic criteria. Investigators have arrived at an algorithm which is outlined in the article by Pimpinelli, cited below. I have reproduced the algorithm which combines clinical, histopathologic, molecular, and immunopathologic findings. In this scoring system, a total of 4 points is required for the diagnosis of mycosis fungoides based on any combination of these four categories.
*Lymphoid atypia is defined as cells with enlarged hyperchromatic nuclei and irregular or cerebriform nuclear contours **PCR/DGGE method (or a related technique such as PCR/temperature gradient gel electrophoresis or PCR/single stranded conformational polymorphism analysis) is preferred with a clonal detection threshold of 1%. ***T-cell antigen deficiency confined to the epidermis. As an example, I have included a clinical photo as well as histologic sections. Based upon the algorithm, these two categories alone sum to a total of 4 points and fulfills the criteria for the diangosis of mycosis fungoides. Thus, if these first two criteria depict an obvious case of mycosis fungoides, additional immunoperoxidase and molecular studies may not be needed. Conversely, since the immunoperoxidase and molecular studies can only sum to a total of 2 points, these findings alone are insufficient to establish the diagnosis. Certain caveats must be emphasized. Finally, one must be careful to define the molecular biological criteria. If a matching clone in multiple skin lesions is identified, this may be strongly associated with mycosis fungoides but may also occur in a clonal dermatitis. Thus clonality was not utilized as a criteria. The PCR/DGGE method is preferred as summarized in the following table.
References: Pimpinelli N, Olsen EA, Santucci M, etal. Defining Early Mycosis Fungoides. J Am Acad Dermatol 2005;53(6):1053-1063. Submitted by Paul K. Shitabata, M.D. |
||||||||||||||||||||||||||||||||||||||||||||||
First Posted on
January 26, 2006
Send Emails to
Webmaster at DermpathMD
Read the Medical Disclaimer