|
|
Regressed Lesions (Melanosis) Regression is both a simple and perplexing topic. The simplicity is identifying the histologic findings of epidermal thinning with loss of the normal rete ridge pattern, papillary dermal fibroplasia, telangiectasia, and melanophages associated with a band-like infiltrate of lymphocytes. The perplexing aspect is what type of lesion was represented at this site before the regression and what should the clinical follow-up be for this lesion? The vast majority of regressed lesions represent melanocytic lesions, usually a regressed melanoma. In another article on this website, I have cautioned against utilizing the term melanoma in situ in the presence of regression. Indeed there is medical literature support of so-called melanoma in situ with regression resulting in metastasis (Guitart J, etal). Additional considerations should include regression in a melanocytic nevus, particularly dysplastic nevi. However, as Dr. LeBoit has correctly pointed out, regression may be seen in non-melanocytic proliferations such as basal cell carcinomas, Bowen's disease, mycosis fungoides, and solar lentigo. I have included a recent case of a basal cell carcinoma illustrating this phenomenon. No prior biopsy or treatment was given to this patient. In figures 1 and 2, there is characteristic thinning of the epidermis with flattening of the rete ridges. Figure 2 illustrates the dermal fibroplasia with melanophages. Adjacent to this area of fibroplasia is a superficial basal cell caricnoma, illustrated in figures 3 and 4. One can easily discern how a diagnosis of a regressed melanocytic neoplasm might be rendered if a small or superficial biopsy of the entire lesion is taken. Thus, what is the appropriate terminology for a regressed lesion, sometimes known as melanosis? I prefer the term regressed lesion and add a clarifying comment. If there is no additional histopathologic clue for the origin of the lesion (ie, no residual atypical junctional melanocytes suggesting a prior melanoma or no epithelial atypia suggestive of Bowen's disease or basal cell carcinoma), my comment will state that regression may be seen in both melanocytic and epithelial neoplasms. Based upon the histopathologic findings seen in this current biopsy, a definitive distinction or diagnosis cannot be rendered as to the origin of this regressed lesion. Thus a complete excision is recommended. I will also comment on the margins and indicate that if the lesion extends to the margins, a complete re-excision is recommended. If the lesion appears completely excised in the plane of section, I will also comment that if any residual lesion still clinically persists, a complete excision is recommended. Submitted by Paul K. Shitabata, M.D. Back To Dermatopathology Accuracy and Concordance References: LeBoit PE. Melanosis and its meanings. Am J Dermatopathol. 2002 Aug;24(4):369-72. Guitart J, Lowe L, Piepkorn M, etal. Histological characteristics of metastasizing thin melanomas: a case-control study of 43 cases. Arch Dermatol. 2002 May;138(5):603-8
|
Last Updated January 23, 2006
Send Emails to
Webmaster at DermpathMD
Read the Medical Disclaimer
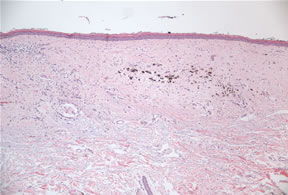
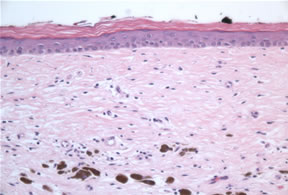
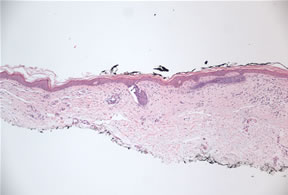
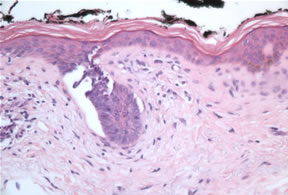 Figure 4
Figure 4