|
|
Image 1-Clinical photograph of patient, taken one week after the biopsy.
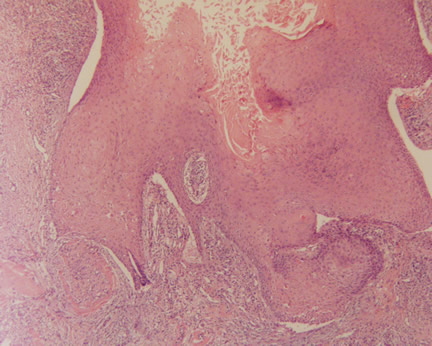
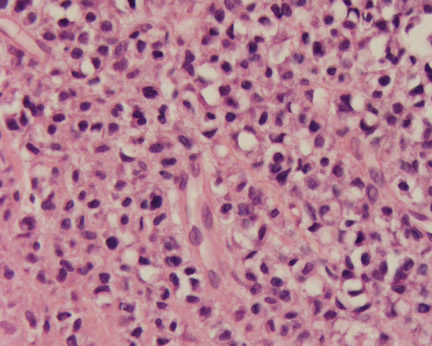
Image 4-In a third focus, there was unusual hyalinization interspersed with the cellular infiltrate.
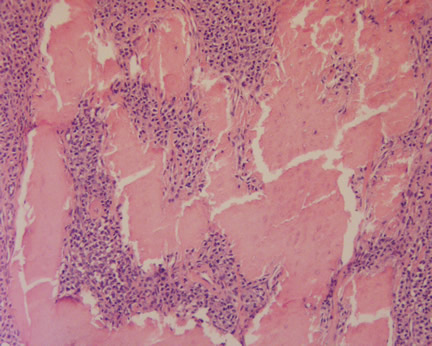
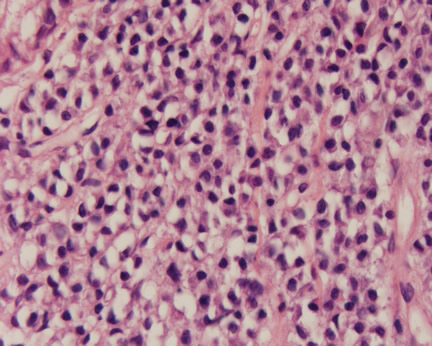
Image 5-The cellular dermal infiltrate contained these atypical cells with a peculiar cytoplasmic clearing, imparting a signet-ring configuration.
|
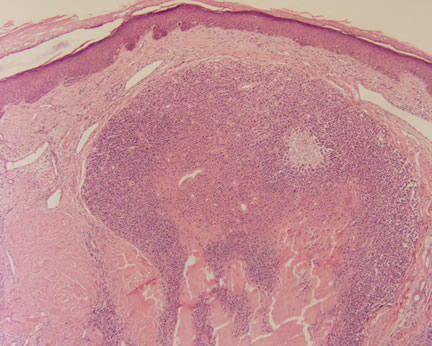
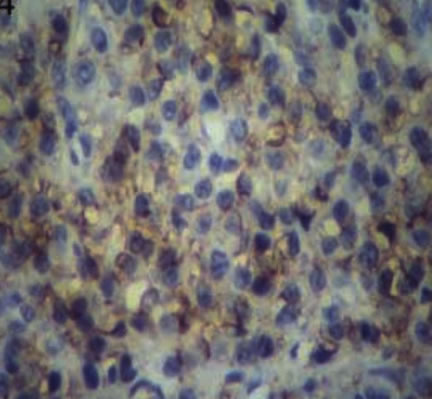
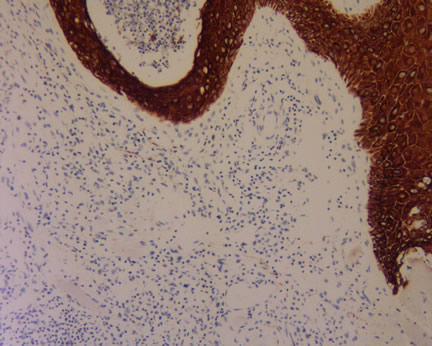
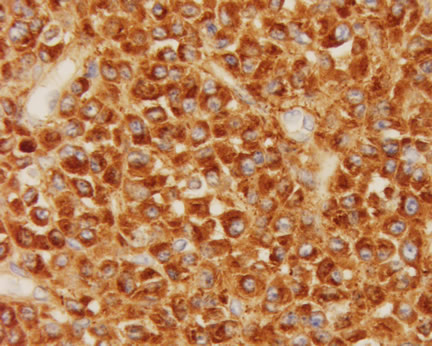
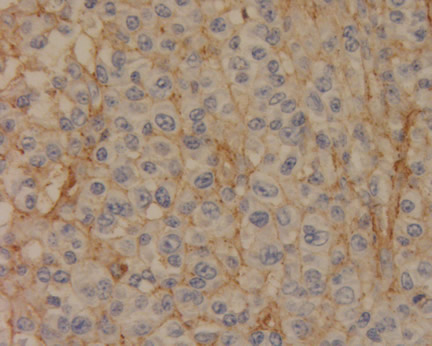
Issues in Dermatopathology We all need consultants. In spite of what some clinical colleagues tell you, we cannot know or be an expert in everything. But what does one do when even the consultants disagree? In January 1998, I reviewed a problematic case taken off the left cheek of a 55 year old Korean man. The lesion was a red plaque measuring about 3 cm. (image 1). He was in otherwise good health. The biopsies presented several unusual histopathologic features (see images 2-6). The epidermis showed irregular hyperpiesia raising the suspicion of a squamous cell carcinoma. The dermal cellular infiltrate had unusual cytological features suggestive of signet rings. Finally, there was a peculiar hyalinization admixed with the cellular infiltrate. When in doubt, dermatopathologists can turn to an armamentarium of special stains and immunoperoxidase studies. Usually, this helps us to narrow our differential diagnosis or confirm a suspected diagnosis. In this case, it only served to obfuscate the diagnosis. Special stains to exclude an unusual infection were negative (mucicarmine, Acid-Fast, PAS, and GMS). Immunoperoxidase studies revealed strong immunostaining for CD31 (Image 7) but were negative for cytokeratins, CEA, smooth muscle actin, S100, HMB45, CD68, and leukocyte common antigen (see image 8). Now we were even more confused! Since the morphology of the cells as well as the clinical presentation did not fit with this latter diagnosis, it was time to send the case to consultants. And now, total chaos ensued! All of the three consultants were expert dermatopathologists, whose names you are all familiar. Their diagnoses are summarized as follows: Consultant 1: Atypical cellular infiltrate, CD31 positive-Pseudoepitheliomatous hyperplasia with atypical mononuclear cells probably representing a malignant neoplasm. Doubt angiosarcoma. Consultant 2: Pseudocarcinomatous hyperplasia with suppuration. Differential diagnosis is between an infectious process such as a deep fungus or atypical mycobacterium, collagenoderma, or even squamous cell carcinoma. He suggested the hyalinzed material could represent bovine collagen (Zyderm) and queried whether the patient received any injections (he didn't). Consultant 3: Atypical cells probably of vascular-endothelial origin with florid pseudo-epitheliomatous hyperplasia and peculiar eosinophilic material interpreted as keratin. (This consultant, in turn, had the case reviewed by two additional dermatopathologist who were equally stymied by the case! He frankly admitted that neither he nor his other colleagues had any idea what this case might represent. He was not even sure if it was benign or malignant.) Now What? In pathology, we sometimes cynically state that if you are unsure of the diagnosis, make sure you send your case to an odd number of consultants, ensuring there will at least be a majority ruling. What does one do when there are three different diagnoses? Through this all, the referring dermatologist tried to calm the frantic patient. The lesion had not changed and he was in otherwise good health. This case was even presented to the Los Angeles Metro Dermatology Society, in hopes that this esteemed gathering of dermatologists would be able to come up with a clear diagnosis. Aside from a few annoyed looks from dermatologists, irritated that a dermatopathologist would present a case with an unknown diagnosis, no answers emerged. About two months later, I received a call from consultant number one. He said that he had still been thinking about the case and remembered another patient of his who had some rare signet ring cells appearing in the dermis, associated with plasma cells. After further evaluation, it was discovered the signet ring cells were plasma cells showing a monoclonal light chain restriction. He thought we should consider an unusual presentation of a cutaneous plasmacytoma and order immunoperoxidase studies for kappa and lambda light chains. Sure enough! The cells lit up with kappa light chain and were negative for lambda light chain (see images 9 and 10). This is histopathologic confirmation of a monoclonal light chain restriction. To complete the story, the patient underwent a bone marrow aspiration and biopsy which was normal with no evidence of a plasma cell dyscrasia. Additional bone scans were negative. A serum and urine protein electrophoresis showed no monoclonal gammopathy and the rest of his serum chemistries, including protein and calcium, were within normal limits. But what about the unusual CD31 staining of the plasma cells? Remember, up to this point, CD31 had been touted as a sensitive and specific marker for endothelial cells. Right about the time of our case, a paper written in a British pathology journal (see reference below), documented a few cases of unusual positive staining by CD31 for...you guessed it, plasma cells! We nor any of the consultants had access to this paper at the time the case presented to us. So, in conclusion, choose your consultants wisely, choose an odd number of consultants, and keep up to date with the medical literature! When you have reviewed the case and discussion, please comment, I will post them anonymously. Submitted by Paul K. Shitabata, M.D. COMMENTS: Nice case and nice presentation. Thanks for sending it on. Who was the consultant who steered you on to the correct plasmacytoma
diagnosis? I'm always impressed by someone who continues to ruminate
about
difficult cases; even more so for those who follow up on their ideas in
a
manner that results in more definitive action. Additional References: The Doctor's Doctor-Plasmacytoma |
Originally Posted August 18, 2005
Send Emails to
Webmaster at DermpathMD
Read the Medical Disclaimer